|
Overview
 It is important to note that pronation is not wrong or bad for you. In fact, our feet need to pronate and supinate to achieve proper gait. Pronation (rolling inwards) absorbs shock and supination (rolling outwards) propels our feet forward. It is our body?s natural shock-absorbing mechanism. The problem is over-pronation i.e. the pronation movement goes too deep and lasts for too long, which hinders the foot from recovering and supinating. With every step, excess pronation impedes your natural walking pattern, causing an imbalance in the body and consequent excessive wear and tear in joints, muscles and ligaments. Some common complaints associated with over-pronation include heel Pain (Plantar Fasciitis), Ball of foot pain, Achilles Tendonitis, Shin splints, Knee Pain, Lower Back Pain. Causes Fallen arches in adults are caused by several things. Below are some of the most common causes. Abnormalities present from birth. Torn or stretched tendons (resulting from foot injuries or foot strains). Inflammation or damage of the PTT (posterior tibial tendon). The PTT is responsible for connecting the middle of the arch to the ankle and lower leg. Dislocated or broken bones (also as a result of injury). Health problems like rheumatoid arthritis. Nerve problems. Other factors like diabetes, obesity, aging and pregnancy (these factors are known to increase the risk of fallen arches). Symptoms A significant number of people with fallen arches (flat feet) experience no pain and have no problems. Some, however, may experience pain in their feet, especially when the connecting ligaments and muscles are strained. The leg joints may also be affected, resulting in pain. If the ankles turn inwards because of flat feet the most likely affected areas will be the feet, ankles and knees. Some people have flat feet because of a developmental fault during childhood, while others may find that the problem develops as they age, or after a pregnancy. There are some simple devices which may prevent the complications of flat feet. Diagnosis Most children and adults with flatfeet do not need to see a physician for diagnosis or treatment. However, it is a good idea to see a doctor if the feet tire easily or are painful after standing, it is difficult to move the foot around or stand on the toes, the foot aches, especially in the heel or arch, and there is swelling on the inner side of the foot, the pain interferes with activity or the person has been diagnosed with rheumatoid arthritis. Most flatfeet are diagnosed during physical examination. During the exam, the foot may be wetted and the patient asked to stand on a piece of paper. An outline of the entire foot will indicate a flattened arch. Also, when looking at the feet from behind, the ankle and heel may appear to lean inward (pronation). The patient may be asked to walk so the doctor can see how much the arch flattens during walking. The doctor may also examine the patient's shoes for signs of uneven wear, ask questions about a family history of flatfeet, and inquire about known neurological or muscular diseases. Imaging tests may be used to help in the diagnosis. If there is pain or the arch does not appear when the foot is flexed, x-rays are taken to determine the cause. If tarsal coalition is suspected, computed tomography (CT scan) may be performed, and if an injury to the tendons is suspected, magnetic resonance imaging (MRI scan) may be performed. flat feet exercises Non Surgical Treatment Treatment isn't usually needed for flat feet because the condition doesn't usually cause any significant problems. Aching feet can often be relieved by wearing supportive shoes that fit properly. You may need to wear shoes that are wider than normal. If your feet overpronate, you may need to wear a special insole (an orthotic) inside your shoes to stop your feet rolling inwards when you walk or run. These will usually need to be made and fitted by a podiatrist. Stretching your calf and Achilles tendon may also help as a tight Achilles can make your foot overpronate. To stretch your calf and Achilles tendon, step forwards with your left leg and bend it, with your right leg straight and both feet pointing forwards, push your right heel into the ground while keeping your right leg straight; you should feel the stretch at the back of your right leg, below the knee, hold the stretch for 15 to 30 seconds and repeat with the opposite leg, repeat the stretch two to four times on each leg, and repeat the overall exercise three to four times a day. Surgical Treatment  Since there are many different causes of flatfoot, the types of flatfoot reconstruction surgery are best categorized by the conditions. Posterior tibial tendon dysfunction. In this condition, the tendon connecting the calf muscle to the inner foot is torn or inflamed. Once the tendon is damaged it no longer can serve its main function of supporting the arch of the foot. Flatfoot is the main result of this type of condition and can be treated by the following flatfoot reconstruction surgeries. Lengthening of the Achilles tendon. Otherwise known as gastrocnemius recession, this procedure is used to lengthen the calf muscles in the leg. This surgery treats flatfoot and prevents it from returning in the future. This procedure is often combined with other surgeries to correct posterior tibial tendon dysfunction. Cleaning the tendon. Also known as tenosynovectomy, this procedure is used in the earlier and less severe stages of posterior tibial tendon dysfunction. It is performed before the arch collapses and while the tendon is only mildly affected. The inflamed tissue is cleaned away and removed from the remaining healthy tendon. Tendon transfer. This procedure is done to correct flatfoot and reform the lost arch in the foot. During the procedure, the diseased tendon is removed and replaced by tendon from another area of the foot. If the tendon is only partially damaged, the inflamed part is cleaned and removed then attached to a new tendon. Cutting and shifting bones. Also called an osteotomy, this procedure consists of cutting and reconstructing bones in the foot to reconstruct the arch. The heel bone and the midfoot are most likely reshaped to achieve this desired result. A bone graft may be used to fuse the bones or to lengthen the outside of the foot. Temporary instrumentation such as screws and plates can also be used to hold the bones together while they heal. Overview
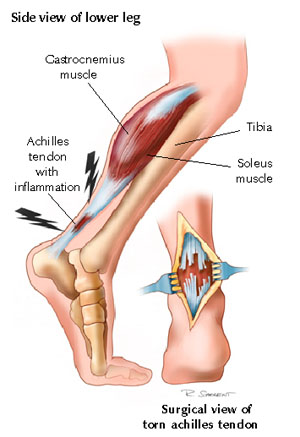 Heel pain can be very aggravating, especially when taking those first steps in the morning. The key to decreasing and possibly eliminating heel pain is to stretch your heel cord and plantar fascia. The heel cord is the Achilles tendon, which connects the gastrocnemius and soleus muscles in the calf to the heel bone. The plantar fascia is a thick tissue that runs along the bottom of your foot, connecting the heel bone to the toes and maintaining the arch. Causes Plantar fasciitis is caused by inflammation and irritation of the tight tissue forming the arch of the foot. The most common cause of heel pain, it typically affects men, aged 40 - 70 who are physically active. The bottom or inside of the foot and / or heel (where heel and arch meet) may hurt or cause severe pain upon standing after resting -- or most often, when arising in the morning. The pain is usually experienced within the first few steps and is often characterized as "walking on nails" or knife blades. The pain may let up after walking a bit but most commonly returns after prolonged movement or a rest. Symptoms The heel can be painful in many different ways, depending on the cause. Plantar fasciitis commonly causes intense heel pain along the bottom of the foot during the first few steps after getting out of bed in the morning. This heel pain often goes away once you start to walk around, but it may return in the late afternoon or evening. Although X-ray evidence suggests that about 10% of the general population has heels spurs, many of these people do not have any symptoms. In others, heel spurs cause pain and tenderness on the undersurface of the heel that worsen over several months. In a child, this condition causes pain and tenderness at the lower back portion of the heel. The affected heel is often sore to the touch but not obviously swollen. Bursitis involving the heel causes pain in the middle of the undersurface of the heel that worsens with prolonged standing and pain at the back of the heel that worsens if you bend your foot up or down. Pump bump, this condition causes a painful enlargement at the back of the heel, especially when wearing shoes that press against the back of the heel. Heel bruises, like bruises elsewhere in the body, may cause pain, mild swelling, soreness and a black-and-blue discoloration of the skin. Achilles tendonitis, this condition causes pain at the back of the heel where the Achilles tendon attaches to the heel. The pain typically becomes worse if you exercise or play sports, and it often is followed by soreness, stiffness and mild swelling. A trapped nerve can cause pain, numbness or tingling almost anywhere at the back, inside or undersurface of the heel. In addition, there are often other symptoms, such as swelling or discoloration - if the trapped nerve was caused by a sprain, fracture or other injury. Diagnosis Your GP or podiatrist (a healthcare professional who specialises in foot care) may be able to diagnose the cause of your heel pain by asking about your symptoms and examining your heel and foot. You will usually only need further tests if you have additional symptoms that suggest the cause of your heel pain is not inflammation, such as numbness or a tingling sensation in your foot - this could be a sign of nerve damage in your feet and legs (peripheral neuropathy), your foot feels hot and you have a high temperature (fever) of 38C (100.4F) or above - these could be signs of a bone infection, you have stiffness and swelling in your heel - this could be a sign of arthritis. Possible further tests may include, blood tests, X-rays - where small doses of radiation are used to detect problems with your bones and tissues, a magnetic resonance imaging (MRI) scan or ultrasound scan, which are more detailed scans. Non Surgical Treatment Heel pain often goes away on its own with home care. For heel pain that isn't severe, try the following. Rest. If possible, avoid activities that put stress on your heels, such as running, standing for long periods or walking on hard surfaces. Ice. Place an ice pack or bag of frozen peas on your heel for 15 to 20 minutes three times a day. New shoes. Be sure your shoes fit properly and provide plenty of support. If you're an athlete, choose shoes appropriate for your sport and replace them regularly. Foot supports. Heel cups or wedges that you buy in the drugstore often provide relief. Custom-made orthotics usually aren't needed for heel problems. Over-the-counter pain medications. Aspirin or ibuprofen (Advil, Motrin IB, others) can reduce inflammation and pain. Surgical Treatment Although most patients with plantar fasciitis respond to non-surgical treatment, a small percentage of patients may require surgery. If, after several months of non-surgical treatment, you continue to have heel pain, surgery will be considered. Your foot and ankle surgeon will discuss the surgical options with you and determine which approach would be most beneficial for you. No matter what kind of treatment you undergo for plantar fasciitis, the underlying causes that led to this condition may remain. Therefore, you will need to continue with preventive measures. Wearing supportive shoes, stretching, and using custom orthotic devices are the mainstay of long-term treatment for plantar fasciitis. heel bursitis Prevention 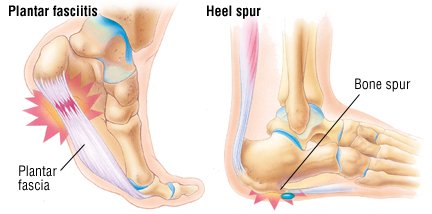 Maintaining flexible and strong muscles in your calves, ankles, and feet can help prevent some types of heel pain. Always stretch and warm-up before exercising. Wear comfortable, properly fitting shoes with good arch support and cushioning. Make sure there is enough room for your toes. Overview
Leg length discrepancies are differences between the lengths of your legs. Not only can the actual difference vary from person to person but also how much it affects daily life. Small discrepancies often go unnoticed and do not need to be treated. Larger differences may affect posture or cause a limp during walking. The discrepancy may be from the upper leg bone (femur) or the lower leg bone (tibia).  Causes LLDs are very common. Sometimes the cause isn?t known. But the known causes of LLD in children include, injury or infection that slows growth of one leg bone. Injury to the growth plate (a soft part of a long bone that allows the bone to grow). Growth plate injury can slow bone growth in that leg. Fracture to a leg bone that causes overgrowth of the bone as it heals. A congenital (present at birth) problem (one whole side of the child?s body may be larger than the other side). Conditions that affect muscles and nerves, such as polio. Symptoms LLD do not have any pain or discomfort directly associated with the difference of one leg over the other leg. However, LLD will place stress on joints throughout the skeletal structure of the body and create discomfort as a byproduct of the LLD. Just as it is normal for your feet to vary slightly in size, a mild difference in leg length is normal, too. A more pronounced LLD, however, can create abnormalities when walking or running and adversely affect healthy balance and posture. Symptoms include a slight limp. Walking can even become stressful, requiring more effort and energy. Sometimes knee pain, hip pain and lower back pain develop. Foot mechanics are also affected causing a variety of complications in the foot, not the least, over pronating, metatarsalgia, bunions, hammer toes, instep pain, posterior tibial tendonitis, and many more. Diagnosis A systematic and well organized approach should be used in the diagnosis of LLD to ensure all relevant factors are considered and no clues are overlooked which could explain the difference. To determine the asymmetry a patient should be evaluated whilst standing and walking. During the process special care should be used to note the extent of pelvic shift from side to side and deviation along the plane of the front or leading leg as well as the traverse deviation of the back leg and abnormal curvature of the spine. Dynamic gait analysis should be conducted during waling where observation of movement on the sagittal, frontal and transverse planes should be noted. Also observe head, neck and shoulder movements for any tilting. Non Surgical Treatment Heel lifts Raise the heel on the shorter leg. It is applied either to the heel of the custom orthotic or to the inside of the shoe under the insole at the heel. Generally if the discrepancy is greater than 3/8 of an inch, the modification is applied externally on the footwear. Custom made orthotics help to provide proper support and alignment to the foot, controlling conditions such as over pronation. Orthopedic Footwear, properly fitted, to which a lift might be applied inside or out.  how can a woman look taller? Surgical Treatment Differences of an inch-and-a-half to two inches may require epiphysiodesis (adjusting the growth of the longer side) or acute shortening of the other side. Differences greater than 2.5 inches usually require a lengthening procedure. The short bone is cut and an external device is applied. Gradual lengthening is done over months to allow the muscles and nerves accommodate the new length. Overview
 This is a painful condition affecting a small nerve in the foot. It occurs when the five long bones that run the length of the foot get pushed together, pinching the nerve in between. This friction on the nerve causes it to thicken and inflame causing pain. The condition gets its name from an American surgeon, George Morton. This is a painful condition affecting a small nerve in the foot. It occurs when the five long bones that run the length of the foot get pushed together, pinching the nerve in between. This friction on the nerve causes it to thicken and inflame causing pain. The condition gets its name from an American surgeon, George Morton.Causes A Morton?s Neuroma are a result of complex biomechanical changes that occur in your feet. There are a number of theories as to the exact cause of the scarring and thickening, but it basically boils down to overload of the tissue structure. The body lays down scar tissue to try to protect the overloaded structure. Tight-fitting shoes may exacerbate a Morton?s Neuroma. Shoes such as high heels and shoes with tight toe boxes (eg womens fashion shoes and cowboy boots) are particularly damaging to the toes. These shoes have a sloping foot bed and a narrow toe box. The slope causes the front of the foot to bear your weight. The angle of the toe box then squeezes your toes together. Footwear is not the only cause of a Morton?s Neuroma. Injuries to the foot can also be a factor in developing the condition by changing your foot biomechanics. Poor foot arch control leading to flat feet or foot overpronation does make you biomechanically susceptible to a neuroma. Symptoms The symptoms of Morton?s Neuroma tend to come and go over time. They are typically exacerbated by physical activity or by wearing certain shoes. Morton?s Neuroma symptoms include sharp pain in the ball of the foot, pain radiating to the tips of the toes, burning pain in the second, third, or fourth toes, numbness in the toes, sensation of a lump between the toes. Diagnosis The physician will make the diagnosis of Morton's neuroma based upon the patient's symptoms as described above in an interview, or history, and a physical examination. The physical examination will reveal exceptional tenderness in the involved interspace when the nerve area is pressed on the bottom of the foot. As the interspace is palpated, and pressure is applied from the top to the bottom of the foot, a click can sometimes be felt which reproduces the patient's pain. This is known as a Mulder's sign. Because of inconsistent results, imaging studies such as MRI or ultrasound scanning are not useful diagnostic tools for Morton's neuroma. Thus the physician must rely exclusively on the patient's history and physical examination in order to make a diagnosis. Non Surgical Treatment Simple treatments may be all that are needed for some people with a Morton's neuroma. They include the following. Footwear adjustments including avoidance of high-heeled and narrow shoes and having special orthotic pads and devices fitted into your shoes. Calf-stretching exercises may also be taught to help relieve the pressure on your foot. Steroid or local anaesthetic injections (or a combination of both) into the affected area of the foot may be needed if the simple footwear changes do not fully relieve symptoms. However, the footwear modification measures should still be continued. Sclerosant injections involve the injection of alcohol and local anaesthetic into the affected nerve under the guidance of an ultrasound scan. Some studies have shown this to be as effective as surgery.  Surgical Treatment The ultimate success of a Morton?s neuroma treated surgically is somewhat unclear. This is likely due to the idea that in most instances a ?Morton?s neuroma? is actually more than just an isolated nerve problem but rather consitutes a metatarsalgia where other structures (such a as the MTP joints) are also problematic, not just the nerve. Therefore, addressing the nerve as well as the other components of a metatarsalgia may offer a better chance of surgical success. However, like many conditions in foot and ankle, it is ideal if this condition can be managed without surgery. Prevention Wearing proper footwear that minimizes compression of the forefoot can help to prevent the development of and aggravation of a Morton's neuroma. There are actually two unique variations of leg length discrepancies, congenital and acquired. Congenital implies that you are born with it. One leg is anatomically shorter in comparison to the other. As a result of developmental stages of aging, the brain picks up on the step pattern and identifies some difference. The entire body usually adapts by tilting one shoulder to the "short" side. A difference of under a quarter inch is not very uncommon, demand Shoe Lifts to compensate and mostly does not have a serious effect over a lifetime.
 Leg length inequality goes typically undiscovered on a daily basis, however this issue is very easily corrected, and can eliminate quite a few cases of lower back pain. Therapy for leg length inequality commonly consists of Shoe Lifts . Many are cost-effective, ordinarily costing less than twenty dollars, compared to a custom orthotic of $200 plus. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position. Low back pain is easily the most widespread ailment impacting men and women today. Around 80 million people experience back pain at some point in their life. It's a problem that costs employers millions of dollars yearly because of lost time and productivity. Fresh and better treatment solutions are always sought after in the hope of minimizing the economical influence this issue causes.  Men and women from all corners of the world suffer from foot ache as a result of leg length discrepancy. In a lot of these cases Shoe Lifts are usually of immense help. The lifts are capable of easing any discomfort and pain in the feet. Shoe Lifts are recommended by many experienced orthopaedic physicians. So that they can support the human body in a balanced fashion, your feet have got a very important job to play. Despite that, it is often the most overlooked area of the body. Some people have flat-feet which means there is unequal force exerted on the feet. This causes other parts of the body including knees, ankles and backs to be impacted too. Shoe Lifts make sure that suitable posture and balance are restored.  Overview The heel bone is the largest bone in the foot and absorbs the most shock and pressure. A heel spur develops as an abnormal growth of the heel bone. Most commonly, calcium deposits form when the plantar fascia pulls away from the heel area, causing a bony protrusion, or heel spur to develop. While bone spurs can develop in other locations such as the rear of the heel bone, this is the most common location for development. The plantar fascia is a broad band of fibrous tissue located along the bottom surface of the foot that runs from the heel to the forefoot. Heel spurs can cause extreme pain in the rearfoot, especially while standing or walking. Causes One frequent cause of heel spurs is an abnormal motion and mal-alignment of the foot called pronation. For the foot to function properly, a certain degree of pronation is required. This motion is defined as an inward action of the foot, with dropping of the inside arch as one plants the heel and advances the weight distribution to the toes during walking. When foot pronation becomes extreme from the foot turning in and dropping beyond the normal limit, a condition known as excessive pronation creates a mechanical problem in the foot. In some cases the sole or bottom of the foot flattens and becomes unstable because of this excess pronation, especially during critical times of walking and athletic activities. The portion of the plantar fascia attached into the heel bone or calcaneous begins to stretch and pull away from the heel bone.  Symptoms Heel spurs are most noticeable in the morning when stepping out of bed. It can be described as sharp isolated pain directly below the heel. If left untreated heel spurs can grow and become problematic long-term. Diagnosis Your doctor, when diagnosing and treating this condition will need an x-ray and sometimes a gait analysis to ascertain the exact cause of this condition. If you have pain in the bottom of your foot and you do not have diabetes or a vascular problem, some of the over-the-counter anti-inflammatory products such as Advil or Ibuprofin are helpful in eradicating the pain. Pain creams, such as Neuro-eze, BioFreeze & Boswella Cream can help to relieve pain and help increase circulation. Non Surgical Treatment Bone spurs rarely require treatment unless they are causing frequent pain or damaging other tissues. Because heel spurs and plantar fasciitis are so closely related, they are usually treated the same way. Symptomatic treatment involves rest, especially from the activity that is contributing to the condition and making symptoms worse (although this may not be easy to discover, as problems can manifest several hours or days after the harmful activity has occurred). If you identify the offending activity, ice is recommended immediately following it. Stretching of the calf muscles after a short warm up is also a good idea and can be helpful. Stretching exercises that gently lengthen the calm muscle will relax the tissue surrounding the heel and should be done several times a day, especially in the morning and after prolonged sitting. Surgical Treatment Usually, heel spurs are curable with conservative treatment. If not, heel spurs are curable with surgery, although there is the possibility of them growing back. About 10% of those who continue to see a physician for plantar fascitis have it for more than a year. If there is limited success after approximately one year of conservative treatment, patients are often advised to have surgery.  Overview Heel spurs are usually under the heel and are generally caused by excessive forces acting on the bone. By far the most common cause of heel spurs is abnormal biomechanics - often the same biomechanics that cause plantar fasciitis. Heel spurs are not a direct cause of heel pain. They grow in response to the forces of the soft tissue pulling on the bone. Any condition where the foot has excessive motion can produce tension within the soft tissues acting on the heel. Causes Early signs of heel pain are usually due to plantar fasciitis, the inflammation of the plantar fascia. It is probably the most common cause of heel pain seen by the podiatrist. It is seen in all groups of people; runners, athletes, weekend warriors, people who have jobs requiring a fair amount of standing, walking, or lifting, and those who have recently gained weight. The pain most often manifests itself after periods of non-weight bearing when the plantar fascia is given a chance to rest, so your first steps cause a sudden strain to the tissue. Pain is most common with the first steps in the morning and after periods of rest. Fortunately, upwards of 80 percent of those treated early do remarkably well with conservative therapy.  Symptoms Heel spurs result in a jabbing or aching sensation on or under the heel bone. The pain is often worst when you first arise in the morning and get to your feet. You may also experience pain when standing up after prolonged periods of sitting, such as work sessions at a desk or car rides. The discomfort may lessen after you spend several minutes walking, only to return later. Heel spurs can cause intermittent or chronic pain. Diagnosis Your doctor, when diagnosing and treating this condition will need an x-ray and sometimes a gait analysis to ascertain the exact cause of this condition. If you have pain in the bottom of your foot and you do not have diabetes or a vascular problem, some of the over-the-counter anti-inflammatory products such as Advil or Ibuprofin are helpful in eradicating the pain. Pain creams, such as Neuro-eze, BioFreeze & Boswella Cream can help to relieve pain and help increase circulation. Non Surgical Treatment Common and effective treatments for Heel Spurs include: Stretching exercises, changing to specific shoes, taping or strapping to rest stressed muscles and tendons, custom orthotic devices and physiotherapy. There are many things you can do to treat heel spurs. You should stretch the muscles and ligaments around the area regularly and ensure you are wearing the right footwear for your feet. There are also tapes and straps that you can apply to the muscles and tendons around the area. For more severe cases, custom orthotics may be the way to go along with aggressive physiotherapy. To treat the pain, over the counter NSAIDs (anti-inflammatory medications) is recommended, but use with caution as prolonged use can lead to the development of ulcers. It is therefore best to apply a topical treatment such as Zax?s Original Heelspur Cream, which contains natural ingredients proven to reduce pain and inflammation. More severe forms of the condition may require corticosteroid injections or surgical procedures, but these are very rare cases. Still, should pain become worse and persist, you should consult with your doctor. Surgical Treatment Almost 90% of the people suffering from heel spur get better with nonsurgical treatments. However, if the conservative treatments do not help you and you still have pain even after 9 to 12 months, your doctor may advise surgery for treating heel spur. The surgery helps in reducing the pain and improving your mobility. Some of the surgical techniques used by doctors are release of the plantar fascia. Removal of a spur. Before the surgery, the doctor will go for some pre-surgical tests and exams. After the operation, you will need to follow some specific recommendations which may include elevation of the foot, waiting time only after which you can put weight on the foot etc. Overview
Retrocalcaneal bursitis is sometimes difficult to differentiate from Achilles tendinitis, at least symptomatically. Both are most uncomfortable during the push-off phase of gait, are most severely painful in the morning and with walking after sitting for a period of time, and generally worsen with activity. Most practitioners make the distinction between the two simply on the basis of location of pain and tenderness. Generally, Achilles tendinitis is felt an inch or two higher than this form of bursitis. Causes Systemic diseases such as rheumatoid arthritis, ankylosing spondylitis, reactive arthritis, psoriatic arthritis, scleroderma, systemic lupus erythematosus, pancreatitis, Whipple disease, oxalosis, uremia, hypertrophic pulmonary osteoarthropathy, and idiopathic hypereosinophilic syndrome have also been associated with bursitis. Symptoms What are the symptoms of heel bursitis? pain, swelling, tenderness, redness, and/or warmth at either the bottom of the heel or top of the heel, depending on the degree of swelling, pain may be a dull ache or substantial enough to cause limping, running, jumping, and walking activities may exacerbate pain, wearing poorly fitting, tight, or high-heeled shoes may exacerbate pain. Diagnosis The diagnosis is based on the symptoms and an examination. For anterior Achilles tendon bursitis, doctors use x-rays to rule out a fracture of the heel bone or damage to the heel bone caused by rheumatoid arthritis or other inflammatory arthritis. Non Surgical Treatment In addition to R.I.C.E., there are a number of other treatments to reduce swelling and any associated pain or discomfort due to heel bursitis. Orthotics or change of footwear. Wearing an orthotic device such as a heel insert can encourage better mechanics in the foot and reduce irritation of the retrocalcaneal bursa. Some people do not need special orthotics but simply need to stop wearing shoes with rigid heel and ankle construction and instead wear more supportive, comfortable shoes. Shoes with an "Achilles notch," a groove in the collar at the back of the shoe to protect the Achilles tendon, can be particularly helpful. (Almost all running shoes are designed with an Achilles notch.) Stretching and physical therapy. Stretching the Achilles tendon often helps alleviate pain. Once the pain is resolved it is important for the patient to continue a regular stretching program. Regular stretching reduces the chance of recurrence. Prevention Maintain proper form when exercising, as well as good flexibility and strength around the ankle to help prevent this condition. Proper stretching of the Achilles tendon helps prevent injury.  Overview OverviewThe smallest four toes of each foot have three bony segments connected by two joints, just as the fingers do. hammertoes is a deformity in which one or more of the small toes develops a bend at the joint between the first and second segments so that the tip of the toe turns downward, making it looks like a hammer or claw. The second toe is affected most often. Causes Certain risk factors increase your likelihood of developing a hammertoe. These include a family history of hammertoes, wearing tight or pointy-toed shoes, wearing shoes that are too small, having calluses, bunions, or corns (thickened layers of skin caused by prolonged/repeated friction) Wearing shoes that are too small can force the joint of your toes into a dislocated position. This makes it impossible for your muscles to stretch out. Over time, the practice of wearing improperly fitting shoes increases your risk of developing hammertoes, blisters, bunions, and corns.  Symptoms SymptomsThe symptoms of hammertoe are progressive, meaning that they get worse over time. Hammertoe causes the middle joint on the second, third, fourth, or fifth toes to bend. The affected toe may be painful or irritated, especially when you wear shoes. Areas of thickened skin (corns) may develop between, on top of, or at the end of your toes. Thickened skin (calluses) may also appear on the bottom of your toe or the ball of your foot. It may be difficult to find a pair of shoes that is comfortable to wear. Diagnosis Hammertoes are progressive, they don?t go away by themselves and usually they will get worse over time. However, not all cases are alike, some hammertoes progress more rapidly than others. Once your foot and ankle surgeon has evaluated your hammertoes, a treatment plan can be developed that is suited to your needs. Non Surgical Treatment In the early stages, the deformities from mallet toe, claw toe and hammertoe can be corrected. But if treatment is delayed too long, permanent stiffness can ensue which can only be corrected by surgery. The most effective treatment options are good fitting footwear. Shoes with a wide toebox will be more comfortable and will reduce the tension on the muscles and friction on the toes. Avoid high heels as they push your feet forwards to the front of the shoes. This increases the pressure on the toes, forcing them to bend more than usual. Shoes should ideally be half an inch longer than your longest toe. Exercises to strengthen and stretch the muscles can be really helpful. Simple things like trying to pick marbles up with hammertoe your feet or scrunching up a towel underneath your foot can work well. Surgical Treatment A variety of anaesthetic techniques are possible. Be sure an discuss this with your surgeon during your pre-op assessment. The type of surgery performed will depend on the problem with your toes and may involve releasing or lengthening tendons, putting joints back into place, straightening a toe and changing the shape of a bone.Your surgeon may fix the toes in place with wires or tiny screws.  Overview OverviewIf you sneak a peek at your feet and notice that your toes are crossed, bent, or just pointing at an odd angle, you probably suffer from a hammertoes. Toes that are scrunched up inside tight shoes or pressed against the toe box of the shoe can bend at the joints and stay that way - resulting in a hammertoe. A hammertoe is a contracture of the toe at one of the two joints in the toe. Due to the pull of the tendons, the joints become more rigid over time. The toe is bent up at the joint and does not straighten out. Causes Hammer toe may also be caused by other medical conditions such as rheumatoid arthritis, osteoarthritis, or stroke because these forms of illnesses involve affectation of the person's muscles and nerves. Diabetes is also a causative factor for hammer toes due to diabetic neuropathy, which often times accompanies advanced instances of diabetes. Injury to a person's toes may also cause hammer toes, particularly if the injury involves breaking of the toes. In some instances, hammer toes may be hereditary. Some people may be genetically predisposed to develop the condition because of the natural structure of their bodies.  Symptoms SymptomsPatients with hammer toe(s) may develop pain on the top of the toe(s), tip of the toe, and/or on the ball of the foot. Excessive pressure from shoes may result in the formation of a hardened portion of skin (corn or callus) on Hammer toes the knuckle and/or ball of the foot. Some people may not recognize that they have a hammer toe, rather they identity the excess skin build-up of a corn.The toe(s) may become irritated, red, warm, and/or swollen. The pain may be dull and mild or severe and sharp. Pain is often made worse by shoes, especially shoes that crowd the toes. While some hammer toes may result in significant pain, others may not be painful at all. Painful toes can prevent you from wearing stylish shoes. Diagnosis The exam may reveal a toe in which the near bone of the toe (proximal phalanx) is angled upward and the middle bone of the toe points in the opposite direction (plantar flexed). Toes may appear crooked or rotated. The involved joint may be painful when moved, or stiff. There may be areas of thickened skin (corns or calluses) on top of or between the toes, a callus may also be observed at the tip of the affected toe beneath the toenail. An attempt to passively correct the deformity will help elucidate the best treatment option as the examiner determines whether the toe is still flexible or not. It is advisable to assess palpable pulses, since their presence is associated with a good prognosis for healing after surgery. X-rays will demonstrate the contractures of the involved joints, as well as possible arthritic changes and bone enlargements (exostoses, spurs). X-rays of the involved foot are usually performed in a weight-bearing position. Non Surgical Treatment Wear sensible shoes. If you don?t want to have surgery to fix your hammertoe, use non-medicated padding along with proper shoes made with a wider and deeper toe box to accommodate your foot?s shape. Ensuring your shoes have a good arch support can slow the progression of the condition as well. Use a pumice stone. The corn or callus that forms on top of the hammertoe can cause discomfort when you wear shoes. Treat the corn by using a file or pumice stone to reduce its size after a warm bath, then apply emollients to keep the area softened and pliable. Use silicone or moleskin padding on top of the area when wearing shoes. Do foot exercises. Theoretically, exercises like extending, then curling the toes, splaying the toes, and moving the toes individually may help prevent the digital contracture that causes hammertoe. Try these suggestions and see what works best for you. Surgical Treatment For severe hammer toe, you will need an operation to straighten the joint. The surgery often involves cutting or moving tendons and ligaments. Sometimes the bones on each side of the joint need to be connected (fused) together. Most of the time, you will go home on the same day as the surgery. The toe may still be stiff afterward, and it may be shorter. If the condition is treated early, you can often avoid surgery. Treatment will reduce pain and walking difficulty.  Prevention PreventionGood circulation is essential. When you're sitting down, put your feet up. If you've been sitting for a while, stretch your legs and feet. Give yourself a foot massage or trade foot massages with someone you love. A warm foot bath is also a good idea. Most people have one foot that's bigger than the other. Fit your shoes to the bigger foot. Buy shoes at the end of the day, as feet tend to swell a bit and you will get a better sense of fit. When buying shoes, wear the socks that you will be using when wearing that shoe. For example, wear an athletic sock when buying athletic shoes and a dress sock when purchasing dress shoes. If the shoe does not feel good at the time of purchase, then it will never feel good. |
